
ACTINIC KERATOSIS (AK)
The full extent of actinic keratosis
isn’t always visible1

Actinic keratosis is the most common precursor of invasive squamous cell carcinoma (iSCC)2,3
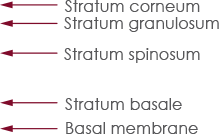
Invasive squamous cell carcinoma can arise directly from any AK lesion—even those limited to the lower third of the epidermis, including the basal layer.4,5
Subclinical AK lesions hidden beneath the surface can pose an unseen threat1,6
AK lesions at any stage, severity, or depth have the potential to progress to iSCC.4,6,7
Subclinical AK lesions can also progress to iSCC1,2,4,7
Prevalence of different pathways of iSCC progression2
(model derived from Fernández-Figueras et al., 2015)
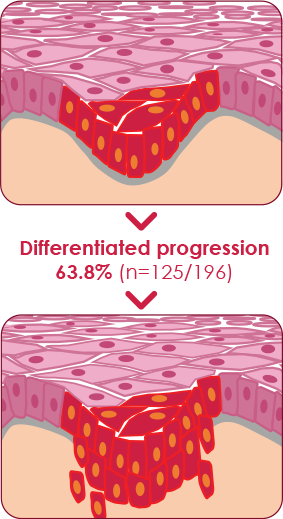
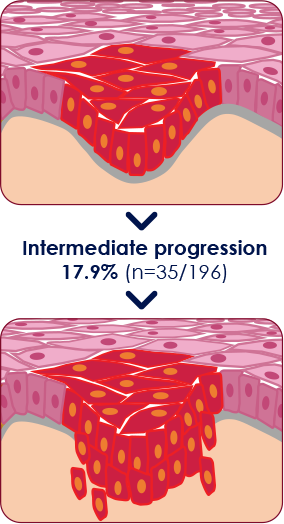
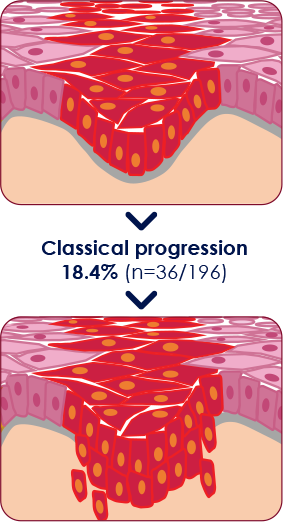
Percentages of histological stages of AK lesions overlying iSCC lesions
This model was derived from results of a relatively small study size of 196 skin biopsy specimens, taken at a single center and does not provide a universal representation of iSCC pathogenesis. Thickness of the epidermal proliferation of atypical keratinocytes overlying the tumor and at its edges was studied. The 196 iSCCs were then assigned to a group (AK I, II, III) depending on the highest AK grade with which they were associated.2

A population at risk
More than a third of the general population over age 51 has at least 1 AK lesion. Those with 10 lesions or more have a 3-fold increase in the risk for progression to skin cancer.8,9
The risk of potential AK progression to iSCC is reported
between 0.025–16%10
Learn how photodynamic therapy may benefit your patients with AK

Schedule a PDT consult to discuss clinical and subclinical and available field options

ACTINIC KERATOSIS (AK)
The full extent of actinic keratosis
isn’t always visible1

Actinic keratosis is the most
common precursor of invasive
squamous cell carcinoma (iSCC)2,3
Invasive squamous cell carcinoma can
arise directly from any AK lesion—even
those limited to the lower third of the
epidermis, including the basal layer.4,5
Subclinical AK lesions hidden
beneath the surface can pose an
unseen threat1,6
AK lesions at any stage, severity, or depth
have the potential to progress to iSCC.4,6,7
Subclinical AK lesions can also progress to iSCC1,2,4,7
Prevalence of different pathways of iSCC progression2
(model derived from Fernández-Figueras et al., 2015)
Percentages of histological stages of AK lesions overlying iSCC lesions
This model was derived from results of a relatively small study size of 196 skin biopsy specimens, taken at a single center and does not provide a universal representation of iSCC pathogenesis. Thickness of the epidermal proliferation of atypical keratinocytes overlying the tumor and at its edges was studied. The 196 iSCCs were then assigned to a group (AK I, II, III) depending on the highest AK grade with which they were associated.2


A population at risk
More than a third of the general population over age 51 has at least 1 AK lesion. Those with 10 lesions or more have a 3-fold increase in the risk for progression to skin cancer.8,9
The risk of potential AK progression to iSCC is reported between 0.025–16%10
Learn how photodynamic therapy may benefit your patients with AK
Schedule a PDT consult to discuss clinical and subclinical and available field options

ACTINIC KERATOSIS (AK)
The full extent of actinic keratosis
isn’t always visible1

Actinic keratosis is the most common precursor of invasive squamous cell carcinoma (iSCC)2,3
Invasive squamous cell carcinoma can arise directly from any AK lesion—even those limited to the lower third of the epidermis, including the basal layer.4,5
Subclinical AK lesions hidden beneath the surface can pose an unseen threat1,6
AK lesions at any stage, severity, or depth have the potential to progress to iSCC.4,6,7
Subclinical AK lesions can also progress to iSCC1,2,4,7
Prevalence of different pathways of iSCC progression2
(model derived from Fernández-Figueras et al., 2015)
Percentages of histological stages of AK lesions overlying iSCC lesions
Percentages of histological stages of AK lesions overlying iSCC lesions
Percentages of histological stages of AK lesions overlying iSCC lesions
This model was derived from results of a relatively small study size of 196 skin biopsy specimens, taken at a single center and does not provide a universal representation of iSCC pathogenesis. Thickness of the epidermal proliferation of atypical keratinocytes overlying the tumor and at its edges was studied. The 196 iSCCs were then assigned to a group (AK I, II, III) depending on the highest AK grade with which they were associated.2

A population
at risk
More than a third of the
general population over
age 51 has at least 1 AK
lesion. Those with 10
lesions or more have a
3-fold increase in the risk
for progression to skin
cancer.8,9
The risk of potential AK progression to iSCC is reported between 0.025–16%10
Learn how photodynamic therapy may benefit your patients with AK
INDICATION AND IMPORTANT SAFETY INFORMATION
INDICATION
AMELUZ® (aminolevulinic acid hydrochloride) topical gel, 10%, a porphyrin precursor, in combination with photodynamic therapy using BF‑RhodoLED® lamp, is indicated for the lesion-directed and field-directed treatment of actinic keratoses of mild-to-moderate severity on the face and scalp.
IMPORTANT SAFETY INFORMATION
AMELUZ® (aminolevulinic acid hydrochloride) topical gel, 10% with BF‑RhodoLED® lamp
AMELUZ®, containing 10% aminolevulinic acid hydrochloride, is a non-sterile gel formulation for topical use only. Not for ophthalmic, oral, or intravaginal use.
AMELUZ®, in conjunction with lesion preparation, is only to be administered by a health care provider. Photodynamic therapy with AMELUZ® involves preparation of lesions, application of the product, occlusion and illumination with BF‑RhodoLED®. The application area should not exceed 20 cm2 and no more than 2 grams of AMELUZ® (one tube) should be used at one time. Lesions that have not completely resolved shall be retreated 3 months after the initial treatment. Refer to BF‑RhodoLED® user manual for detailed lamp safety and operating instructions. Both patient and medical personnel conducting the PDT should adhere to all safety instructions.
AMELUZ® shall not be used by persons who have known hypersensitivity to porphyrins or any of the components of AMELUZ®, which includes soybean phosphatidylcholine. AMELUZ® should also not be used for patients who have porphyria or photodermatoses.
Hypersensitivity reactions have been reported with the use of AMELUZ® prior to photodynamic therapy (PDT). AMELUZ® should be washed off and appropriate therapy instituted. Inform patients and their caregivers that AMELUZ may cause hypersensitivity, potentially including severe courses (anaphylaxis).
Transient Amnestic Episodes have been reported during postmarketing use of AMELUZ® in combination with photodynamic therapy (PDT). If patients experience amnesia or confusion, discontinue treatment. Advise them to contact the healthcare provider if the patient develops amnesia after treatment.
Eye exposure to the red light of the BF‑RhodoLED® lamp during PDT must be prevented by protective eyewear. Direct staring into the light source must be avoided. AMELUZ® increases photosensitivity. Patients should avoid sunlight, prolonged or intense light (e.g., tanning beds, sun lamps) on lesions and surrounding skin treated with AMELUZ® for approximately 48 hours following treatment whether exposed to illumination or not.
AMELUZ® has not been tested on patients with inherited or acquired coagulation disorders. Special care should be taken to avoid bleeding during lesion preparation in such patients. Any bleeding must be stopped before application of the gel. AMELUZ® should not be used on mucous membranes or in the eyes.
Local skin reactions at the application site were observed in about 99.5% of subjects treated with AMELUZ® and narrow spectrum lamps. The very common adverse reactions (≥10%) during and after PDT were application site erythema, pain/burning, irritation, edema, pruritus, exfoliation, scab, induration, and vesicles. Most adverse reactions occurred during illumination or shortly afterwards, were generally of mild or moderate intensity, and lasted for 1 to 4 days in most cases; in some cases, however, they persisted for 1 to 2 weeks or even longer. Severe pain/burning occurred in up to 30% of treatments.
There have been no formal studies of the interaction of AMELUZ® with other drugs. Concomitant use of the following photosensitizing medications may increase the phototoxic reactions after PDT: St. John’s wort, griseofulvin, thiazide diuretics, sulfonylureas, phenothiazines, sulphonamides, quinolones, and tetracyclines.
There are no available data on AMELUZ® use in pregnant women to inform a drug associated risk. No data are available regarding the presence of aminolevulinic acid in human milk, the effects of aminolevulinic acid on the breastfed infant or on milk production. Safety and effectiveness in pediatric patients below the age of 18 have not been established as AK is not a condition generally seen in the pediatric population. No overall differences in safety or effectiveness were observed between elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Please read the US Full Prescribing Information for AMELUZ® and/or US User Manual of BF‑RhodoLED® lamp available together at https://www.ameluz.com/PI.
You are encouraged to report side effects of AMELUZ®. Please contact Biofrontera Inc. at 1‑844‑829‑7434 or FDA at 1‑800‑332‑1088 or www.fda.gov/medwatch.
References: 1. Berman B, Amini S, Valins W, Block S. Pharmacotherapy of actinic keratosis. Expert Opin Pharmacother. 2009;10(18):3015-3031. 2. Fernández-Figueras MT, Carrato C, Sáenz X, et al. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J Eur Acad Dermatol Venereol. 2015;29:991-997. 3. Criscione V, Weinstock M, Naylor M, Luque C, Eide M, Bingham S. Actinic keratoses natural history and risk of malignant transformation in the veterans affairs topical tretinoin chemoprevention trial. Cancer. 2009;115:2523–2530. 4. Fernandez Figueras MT. From actinic keratosis to squamous cell carcinoma: pathophysiology revisited. J Eur Acad Dermatol Venereol. 2017;31(Suppl 2):5-7. 5. Siegel JA, Korgavkar K, Weinstock MA. Current perspective on actinic keratosis: a review. Br J Dermatol. 2017;177(2):350-358. 6. Stockfleth E. The importance of treating the field in actinic keratosis. J Eur Acad Dermatol Venereol. 2017;31(Suppl 2):8-11. 7. Schmitz L, Novak B, Hoeh AK, Luebbert H, Dirschka T. Epidermal penetration and protoporphyrin IX formation of two different 5-aminolevulinic acid formulations in ex vivo human skin. Photodiagnosis Photodyn Ther. 2016;14:40-46. 8. Flohil C, van der Leest R, Dowlatshahi E, Hofman A, de Vries E, Nijsten T. Prevalence of actinic keratosis and its risk factors in the general population: the Rotterdam Study. J Invest Dermatol. 2013;133(8):1971-1978. 9. de Berker D, McGregor JM, Mohd Mustapa MF, Exton LS, Hughes BR. British Association of Dermatologists’ guidelines for the care of patients with actinic keratosis 2017. Br J Dermatol. 2017;176(1):20-43. 10. Fuchs A, Marmur E. The kinetics of skin cancer: progression of actinic keratosis to squamous cell carcinoma. Dermatol Surg. 2007;33(9):1099-1101.